,
by Carmen Phillips
Scientists have devised a potential new strategy for treating cancer by taking the ability of tumors to rapidly evolve and turning it against them.
The particular evolutionary change they’re targeting is tumors’ uncanny capacity for making tiny changes in their biological makeup that can cause a cancer drug that had been working to stop doing so—a phenomenon often called treatment resistance.
But the researchers, from Penn State, have come up with a way to take advantage of this troublesome adaptation. And, surprisingly, it involves intentionally engineering cancer cells within a tumor to be resistant to a specific treatment from the get-go.
Their idea is that as a patient undergoes treatment, the engineered cancer cells don’t just survive, they thrive, quickly taking over the tumor. And that’s when the tables turn, because those same cancer cells are also engineered to have a second skill: producing a drug that kills both them and other nearby, nonengineered cancer cells.
By giving or stopping the use of specific drugs, the engineered cells’ new abilities can be turned on and off like light switches, explained the study’s lead investigator, Justin Pritchard, Ph.D., of Penn State’s Huck Institutes of the Life Sciences.
In experiments in mouse models of lung cancer, the approach worked precisely as hoped, with tumors being completely eradicated and appearing not to return. The study, funded in part by NCI and several other NIH institutes, was published July 4 in Nature Biotechnology.
Khalid Shah, Ph.D., director of the Center for Stem and Translational Immunotherapy at Brigham and Women’s Hospital, who has led research on engineering cancer cells to use them as cancer therapy, called the results “promising.” The findings, Dr. Shah said, provide strong evidence it’s possible to “forward engineer the evolution of tumor cells.”
“We know that it’s a different way” to think about treating cancer, Dr. Pritchard said. But with these promising initial results, he continued, their team feels like “there are a lot of opportunities here.”
The evolution of treatment resistance
Treatment resistance is among the biggest challenges in cancer, with some studies estimating that it contributes to 80% to 90% of cancer-related deaths.
Cancer cells that become resistant to a treatment, or that are naturally resistant, are much like a handful of weeds in a lawn that, unlike others in the yard, aren’t killed by weed spray from the local hardware store. In a matter of days or weeks, those few stubborn weeds can seed a lot of friends throughout the lawn.
Similarly, in tumors, cancer cells that are sensitive to a treatment are killed off, while those that have the biological wherewithal to withstand those assaults remain. Those resistant cells then start multiplying and the tumor resumes growing.
Precisely how individual tumors become resistant can vary from person to person, but often there are common mechanisms—most often new genetic changes—that cancer cells acquire. This is particularly true for resistance to targeted therapies, which represent the vast majority of new cancer drugs approved by the Food and Drug Administration over the past 25 years.
For example, targeted therapies work by latching on to part of a mutated protein on or inside cancer cells, which in turn creates a cascade of events that causes the cells to die.
But as tumors are barraged by these therapies, over time some cells in the tumor develop additional genetic mutations that cause the shape of the proteins at those precise binding spots to change. When that happens, the drugs can no longer grab on to their protein targets on those cells, and soon enough the treatments stop working altogether.
The solution to this problem has been for researchers to develop new forms of targeted therapies (often called second- and third-generation drugs) that can work even when resistance-inducing genetic changes are present in those cells.
Many of these next-generation therapies “are great drugs,” Dr. Pritchard said. But, he added, tumors almost always find a way to outwit them too.
Redirecting tumor evolution
The Penn State team decided to revisit this “reactive” strategy to combatting resistance. Instead of waiting to see how tumors evolve to escape the assaults of a given treatment, they thought, why not “redirect” evolution and use it in their favor?
To pull off this redirection, they would use genetic engineering technology to insert two different genes into cancer cells in the lab that would give them specific abilities.
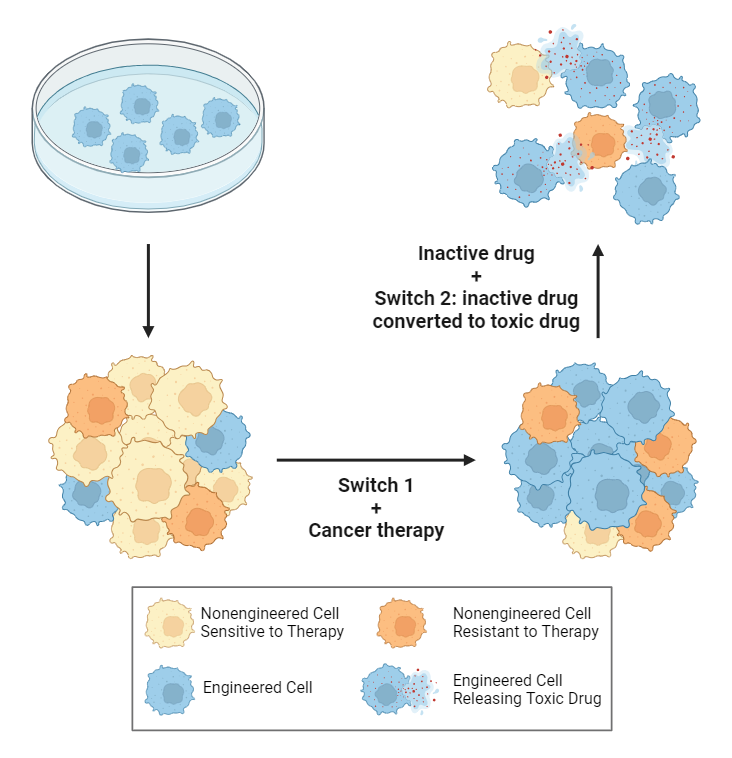
In this “forward engineering of tumor evolution” strategy, after cancer cells with specific genetic changes are in a tumor, drugs are used to activate those two genes (switch 1 and switch 2), ultimately killing the tumor.
Credit: NCI/Created with Biorender.com
The first gene, or switch 1, provides the instructions for making the cells resistant to a specific treatment.
The second gene, or switch 2, transforms the cells into “local drug factories,” providing the instructions for transforming an inactive drug into a toxic drug. After killing the cancer cells, that toxic drug is also dispersed into their nearby surroundings, killing other cancer cells in the immediate area.
For the strategy to work, this collateral damage—or bystander effect—to nearby cancer cells is critical, wrote Andriy Marusyk, Ph.D., who studies cancer evolution at Moffitt Cancer Center in Tampa, FL, in an editorial that accompanied the study.
The bystander effect “maximizes the odds of” eliminating nonengineered cancer cells, Dr. Marusyk wrote, but also “engineered cells in which [the gene for switch 2] was lost or inactivated by mutations.”
Eliminating tumors in mice
To test the feasibility of their idea, Dr. Pritchard and his team began by using computer models that allowed them to better understand how tumors evolve in response to different treatments. Those models, and some laboratory experiments, also helped them simulate the impact of their strategy in different cancer types using different therapies and gene designs for the switches.
A big part of this work, Dr. Pritchard said, was “thinking about all the different ways this [strategy] could go wrong.”
From there, they again used the computer model to help design a switch strategy for a common treatment scenario: lung cancer with mutations in the EGFR gene being treated with the third-generation EGFR-targeted therapy osimertinib (Tagrisso). Although studies show that treatment with osimertinib shrinks tumors for extended periods in about 70% of people treated with it, resistance invariably sets in and the tumors resume growing.
They then tested the strategy in mice. To get the engineered cells into tumors, both engineered and nonengineered EGFR-mutated cancer cells (including those naturally resistant to osimertinib) were implanted into mice, which in short order formed into tumors.
Switch 1 was turned on by giving the mice a drug called a dimerizer, while switch 2 was turned on by the inactive drug that would be turned into a toxin.
Initial experiments showed that the strategy shrank tumors and appeared to have the desired bystander effect. For the final experiments, the teams developed mice with tumors that better simulate those in humans, in that they had more cells that were naturally resistant to osimertinib.
Ten mice were not implanted with any engineered cancer cells and 12 had tumors that did form in part from implanted engineered cells.
In the group of 10 mice, treatment with osimertinib initially shrank tumors in all of them. But the tumors soon began growing again and all the mice quickly died. By contrast, 11 of 12 mice with engineered cells in their tumors were alive several months after starting treatment with osimertinib with no obvious evidence that the tumors had started growing again.
The challenge of moving from the lab to patients
There’s a lot more research to be done, Dr. Shah said. But this initial work shows that it’s possible to force “drug resistance in a direction that is more favorable for treatment as opposed to allowing tumors to develop resistant [cancer cell] populations randomly.”
Moving this idea from success in mice to testing in humans will be difficult, Dr. Pritchard acknowledged. Although there are several obstacles, he believes the biggest “is delivery”—that is, getting the engineered cancer cells into tumors.
Instead of engineering cells in the lab and then giving them back to patients, one potential option, Dr. Marusyk noted, involves a lesson from COVID vaccines: using mRNA technology to deliver the instructions for the switches directly to tumors.
With continued advances in different ways of transferring genetic information into cells, he wrote, getting the switches into cancer cells in the body “is not an insurmountable challenge.”
Dr. Shah pointed to other potential hurdles. For example, the percentage of cells in a tumor that are inherently resistant to a given treatment is an important consideration, he continued. Levels of these cells “vary across different tumor types and patients,” he explained, and will likely affect the engineered cells’ ability to take over a tumor.
So, getting the right mix of engineered cells to resistant cells in a given tumor will be “crucial for the strategy’s success,” Dr. Shah said.
According to Dr. Pritchard, the Penn State researchers are moving forward with testing strategies for delivering the genes for the switches to tumors and fine-tuning the approach in more advanced animal models. They’re also considering which types of cancers would be best to focus on initially in future human studies.
“We’re thinking about that a lot,” Dr. Pritchard said. Given the unique nature of their strategy, he continued, selecting the right situation for initial human studies “will be very important.”


{kind=link}