The placenta can be considered the powerhouse of pregnancy. It’s an intricate network of vessels and tissues that nourishes and sustains developing life.6 But what happens when the placenta isn’t located where it should be? Let’s discuss the symptoms and complications that can occur when the placenta blocks your baby’s exit from your uterus (placenta previa). We’ll also go over whether there’s a treatment for placenta previa and what questions to ask your doctor about it.
Placenta previa occurs when a developing placenta’s position entirely or partially covers the cervical opening. Unfortunately, this blockage can prevent a safe path for vaginal birth and increases the risk of dangerous bleeding during pregnancy. This condition affects approximately 0.3-2% of pregnancies in the third trimester.1
The good news? The placenta can move within your uterus. Up to 90% of low-lying placenta previas will resolve by delivery as the uterus expands and the placenta grows.1
There are three types of placenta previa:1
- Marginal or “low lying” placenta previa: This is a placenta lying within 2 centimeters of the internal cervical opening. This type is the most likely to migrate away from the cervical opening, also called the cervical os.
- Partial placenta previa: The placenta partially blocks the internal cervical opening.
- Total or complete placenta previa: The placenta completely blocks the internal cervical opening.
A transvaginal ultrasound examination determines the position of your placenta in relation to the cervical os.1,4
Placenta previa can be diagnosed early in pregnancy by routine transvaginal ultrasound. A follow-up ultrasound between 28 and 32 weeks can determine if the placenta previa is persistent and unlikely to move.1,4
Healthcare providers may suspect placenta previa if you develop painless, bright red vaginal bleeding in the second or third trimesters. However, placenta previa is just one of several conditions that may cause vaginal bleeding in later gestation. The cardinal placenta previa symptom of painless bleeding may begin after intercourse, after a vaginal exam, during labor, or due to no identifiable cause.1
Causes and Risk Factors
The causes of this condition are mainly unknown. However, several risk factors have been identified:1
- Age greater than 35 years old
- Multiple pregnancies
- Assisted reproductive technology
- Smoking
- Cocaine use
- History of suction and curettage
- History of previous cesarean sections
- History of previous placenta previa
These risk factors may result in endometrial damage, uterine scarring, or abnormal placental blood flow.1 This impacts how the placenta grows and connects to the inside of the uterus. Certain risk factors may increase the chance of developing this condition, but they don’t guarantee the development of it.1
Placenta previa will change the care you receive during pregnancy and delivery, and significant complications are possible. Open communication with your obstetric provider is paramount. Here are the potential complications:
This condition can significantly increase the risk of preterm delivery. A study revealed that 3.5% of pregnancies delivered before 28 weeks, 11.7% delivered before 32 weeks, and 16.1% delivered before 34 weeks.2
A baby delivered preterm can have several complications depending on the gestational age. Regrettably, placenta previa is associated with a three- to four-fold increase in infant death that’s generally due to the risks associated with early preterm delivery.1 Other risks for the newborn include:1
- Low birth weight
- Low APGAR score
- Respiratory distress syndrome
Thankfully, research hasn’t found placenta previa to impact infant growth.7
Bleeding from placenta previa can lead to life-threatening hemorrhage and occurs in nearly 60% of pregnancies complicated by placenta previa.2 Maternal hemorrhage can lead to:2
- Blood transfusion
- Intensive care unit admission
- Septicemia-bacterial infection of the blood
- Hysterectomy (removal of the uterus)
- Death
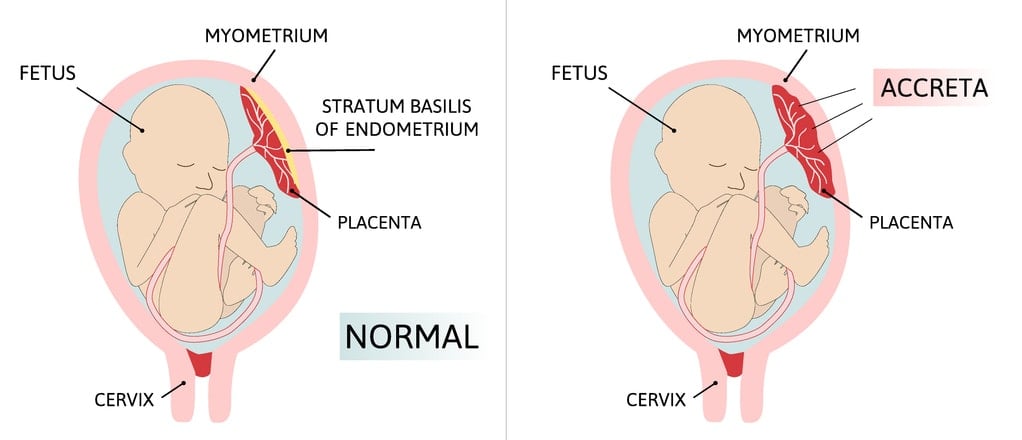
Placenta accreta spectrum (PAS) occurs when the placenta grows into the uterus’ myometrium or inner lining. You’ll be at a greater risk of developing PAS if you have placenta previa.3
The placenta accreta spectrum describes the depth at which the placenta has grown into the myometrium. PAS significantly increases the pregnant parent’s risk for life-threatening bleeding, hysterectomy, and death.3 Additionally, if you have placenta previa and a history of previous cesarean section, your risk of developing PAS increases with each cesarean section.3
Unfortunately, there’s no confirmed treatment for placenta previa.3 It’s a condition of active and expectant management. Medical intervention depends on the extent of placenta previa, the number of weeks pregnant, the presence of bleeding, the beginning of labor, and any other complicating factors. The delivery plan for patients with this condition is cesarean section between 36-37 weeks gestation.8
In the past, bed rest and pelvic rest (no intercourse) may have been considered placenta previa self-care. However, there’s limited modern research to support the benefit of these restrictions.3 In fact, limiting physical activity may increase the risk of blood clots, bone weakening, and a decrease in muscle mass.5 Your provider can tailor any “restrictions” based on your situation while considering the extent of the previa, weeks of gestation, and presence of bleeding.
Finding out you have placenta previa can be overwhelming. You may have lots of questions to ask your obstetric provider. Here are some good ones to begin the conversation:2
- Is a vaginal birth possible with placenta previa?
- What symptoms of placenta previa during pregnancy require an immediate phone call and/or hospital visit?
- Will my delivery be scheduled, or do I wait for labor to start?
- Will a blood transfusion be necessary?
- Do the options for anesthesia during delivery change?
- What additional medical interventions may I expect? (example: two intravenous lines or prophylactic medications)
- How can I ensure proper bonding with my baby during and after a cesarean delivery?
The complications of this condition can be severe, so life-saving measures and giving consent will likely be an essential part of your discussions with your obstetric provider.
Placenta previa, especially partial or complete placenta previa, comes with important considerations for pregnancy and delivery. Although there’s no treatment for placenta previa, knowing the risks and potential outcomes of this condition will help make you more prepared. Don’t hesitate to speak to your obstetric provider about what to expect!


{kind=link}